Community mobilizers discuss vaccination with the teachers of a Quranic School, who agree to allow mass immunization of their students (Sokoto State, northern Nigeria). UNICEF/Nigeria/Andriamasinoro
8 November 2012 – The crisis in Africa’s Sahel region continues. According to the Food and Agriculture Organization, 18.7 million people face food and nutrition insecurity and more than a million children under five years of age are at risk of severe acute malnutrition. With refugees continuing to file into camps across the region, the risk of an outbreak is heightened. Undernourished people, close quarters and a lack of flushing toilets mean that camp conditions are almost perfect for diseases like polio to spread.
So this is a bad time for immunization rates in the border state of Sokoto, Nigeria to be falling. Poliovirus from Sokoto has a history of travelling across borders and infecting neighbouring countries – including some of those worst-hit by the crisis. Yet the state has reported a worrying decrease in population immunity, with almost a third of all children under five recorded as being under-immunized. Lot Quality Assurance Sampling (LQAS) data from recent polio vaccination campaigns has shown a steady decline in children being vaccinated since May. And while Sokoto has reported a deceptively low eight cases so far this year, environmental surveillance regularly detects wild poliovirus and the state has reported a case of circulating vaccine-derived poliovirus type 2 – sure signs that too few children are immunized.
Previously primarily concerned with the obvious troubles of Katsina and Kano states, the world of polio eradication is now turning its attention to Sokoto, focusing on improving the quality of polio vaccination campaigns in the state – including through the use of Global Information Systems (GIS) mapping technology. And to help prevent the spread of the virus across borders, polio vaccine continues to be administered periodically at refugee camps, while funding has been scraped together for two multi-country polio vaccination rounds across west Africa – one of which took place at the end of October with another to take place on the 23-26 November.
National Supplementary Immunization Team Leader Dr Pankaj Bhatnagar sharing experienceswith vaccinators and supervisors in Nigeria. UNICEF/India
National Supplementary Immunization Team Leader Dr Pankaj Bhatnagar sharing experiences with vaccinators and supervisors in Nigeria.UNICEF/India
When India was officially removed from the list of polio-endemic countries in February 2012, three challenges became clear: the need to maintain extremely high levels of immunity to polio until the virus was eradicated globally, the need to be prepared for any importation and the need to share India’s rich experience in stopping transmission in one of the world’s most persistent and virulent reservoirs of wild polio virus with remaining endemic, re-established transmission and outbreak countries.
For years, India had been the world’s largest exporter of wild polio virus, having exported polio to central Asia, Africa (twice) and regularly to its near neighbours including Bangladesh and Nepal. Those episodes of exportation posed a real threat to the programme – if India’s large travelling population could export polio so regularly, then clearly it could import polio back along those same routes.
The Independent Monitoring Board (IMB) of the Global Polio Eradication Initiative in its January 2012 report put it succinctly: “Ultimately, the children of India will be completely safe from polio only when it is eradicated globally.”
The IMB in its report, called upon the India polio eradication programme to support polio-infected countries through the application of lessons learned: “If India knew 10 years ago what it knows now, it would have been able to stop transmission more quickly,” the report said. “We hope that the programme can now find some energy to assist other countries’ programmes.”
The India programme has embraced this call, sending staff to support remaining endemic countries, hosting visits from neighbouring Governments and from within the polio partnership, and sharing programmatic best practices, including: programme management, methods to maximize coverage during rounds, media advocacy strategies, monitoring and evaluation formats, communication and training materials, and ground-level tools to increase the effectiveness of front-line vaccinators and social mobilizers.
Read the India Communication Update about India’s cooperation and support across operational and communication issues for the remaining endemic countries.
President Karzai of Afghanistan, President Zardari of Pakistan, B. Gates, Gates Foundation, polio survivor R. Ferris, President Jonathan of Nigeria, W.J. Wilkinson, chair Rotary Foundation Trustees, and Dr M.Chan, Girector-General of WHOStuart Ramson/Insider Images
UNITED NATIONS, 27 September 2012 – In a display of solidarity, leaders from around the world today vowed to capitalize on progress achieved this year and to step up the fight to eradicate polio. Heads of state from Afghanistan, Nigeria and Pakistan stood alongside donor government officials and new donors from the public and private sector to outline what is needed to stamp out this disease forever: long-term commitment of resources, applying innovative best practices, and continued leadership and accountability at all levels of government in the endemic countries.
“This decisive moment is a matter of health and justice. Every child should have the right to start life with equal protection from this disease. That’s why I have made eradicating polio a top priority for my second term as Secretary-General,” said UN Secretary-General Ban Ki-moon.
Polio is a vaccine-preventable disease that is more than 99 percent eliminated from the world. Today, there are the fewest number of polio cases in the fewest districts in the fewest countries than at any time in history. In 1988, when the global fight against polio began, there were 125 countries where polio raged. Today, there are only three: Nigeria, Pakistan and Afghanistan. India, long-regarded as the nation facing the greatest challenges to eradication, has been polio-free for more than 18 months.
“The evidence is clear: if we all do our part, we can and will end this disease. But we must act quickly and give ourselves the very best chance to succeed,” said Bill Gates, co-chair of the Bill & Melinda Gates Foundation, one of the leading donors to the Global Polio Eradication Initiative (GPEI). “When we defeat polio, it will motivate us to aim for other great health and development milestones.”
Earlier this year, at the World Health Assembly, 194 member states declared the completion of polio eradication to be a “programmatic emergency for global public health.” In order to look beyond short-term challenges, however, GPEI is developing a long-term roadmap for ending polio. The strategy also will ensure that the legacy of investments in polio supports other vaccine-preventable disease goals.
“Failure to eradicate polio is unforgiveable, forever. Failure is not an option. No single one of us can bring this long, hard drive over the last hurdle. But together we can,” said Dr. Margaret Chan, Director-General of the World Health Organization.
Ending polio is an important early milestone in the Decade of Vaccines, a global vision and commitment to reach all children with the vaccines they need. A polio-free world also will lay the foundation for a better public health system that provides critical health services for children in the poorest and most inaccessible places.
“Together we can make history by eradicating polio – thanks mostly to the heroes in the field who risk their lives, every day, to deliver vaccines to children in some of the most dangerous parts of the world,” said Anthony Lake, UNICEF Executive Director.
The high-level event, “Our Commitment to the Next Generation: The Legacy of a Polio-free World,” featured opening remarks from UN Secretary-General Ban Ki-moon and was moderated by Senator Timothy E. Wirth, president of the UN Foundation.
Speakers included leaders of the three polio-endemic countries: President Hamid Karzai, Islamic Republic of Afghanistan; President Goodluck Jonathan, Federal Republic of Nigeria; and President Asif Ali Zardari, Islamic Republic of Pakistan. Earlier this year, these leaders launched national emergency plans to stop transmission of polio in their countries.
“Governments need to step up and honor their commitments to polio eradication if we are to achieve a polio-free world,” said Wilfrid J. Wilkinson, Chair of Rotary Foundation Trustees. “We must seize the advantage by acting immediately, or risk breaking our pledge to the world’s children.” Rotary International, which already has contributed US$1.2 billion to polio eradication, announced additional funding of $75 million over three years to GPEI.
Australian Prime Minister Julia Gillard reinforced Australia’s commitment and called on the Commonwealth to do its part. Last October, Australia committed $50M during the Commonwealth Heads of Government Meeting. Also speaking was Kathleen Sebelius, Secretary of Health and Human Services for the United States. The United States has been the leading donor to the GPEI and provides technical support through the US Centers for Disease Control & Prevention (CDC).
“We have been given the unique opportunity to end polio and provide a lasting legacy for the world’s children,” said Dr. Thomas Frieden, Director of the CDC. “Together we must strive to achieve this important global milestone.”
The Islamic Development Bank, a new donor to the polio eradication effort, announced a three-year $227 million financing package to Pakistan which will cover the majority of the country’s polio vaccination campaign costs. It also announced a $3 million grant for polio eradication activities in Afghanistan.
Additional leaders pledged new and continued commitment to polio eradication. These included:
H.E. Julian Fantino, Minister, International Cooperation, Canada, who announced an initiative to engage civil society to match funds to GPEI;
Rt. Hon. Alan Duncan, Minister of State, International Development, United Kingdom, whose government committed an additional £25M to polio eradication in 2012;
Mr. Sandro Rosell, President, Football Club Barcelona (FCB) and FCB Foundation, who announced the club’s engagement on the polio issue in collaboration with the Gates Foundation and Etisalat, the largest telecomm operator in the Middle East;
Ms. Aseefa Bhutto Zardari, Pakistan’s Goodwill Ambassador on Polio Eradication.
On 29 September, the Global Poverty Project, a campaign group aimed at ending extreme poverty, will host the Global Citizen Festival, a concert bringing together more than 60,000 people in New York’s Central Park with the aim of inspiring a global movement to voice support for eradicating polio and ending extreme poverty.
The Global Polio Eradication Initiative (GPEI), launched in 1988, is spearheaded by national governments, the World Health Organization (WHO), Rotary International, the US Centers for Disease Control and Prevention (CDC) and UNICEF, and supported by key partners including the Bill & Melinda Gates Foundation.
Since its launch, the incidence of polio has been reduced by more than 99 percent. In 1988, more than 350,000 children were paralyzed each year in more than 125 endemic countries. In 2012, 145 new cases have been reported, and only three countries remain endemic: Nigeria, Pakistan and Afghanistan.
Bill & Melinda Gates Foundation: media@gatesfoundation.org, +1 206 709 3400
Rotary International: Petina Dixon-Jenkins. petina.dixon@rotary.org, +1 847 866 3054
UNICEF: Christian Moen. cmoen@unicef.org, +1 212 326 7516 or mobile +1 917 299 1041
US CDC: Alan Janssen. axj3@cdc.gov, +1 404 639 8517
WHO: Sona Bari. baris@who.int, +41 22 791 1476 or mobile +41 79 475 5511
Vaccinator administering the Oral Polio Vaccine during the May 2012 Immunization Plus Days. UNICEF Nigeria/2012/Andriamasinoro
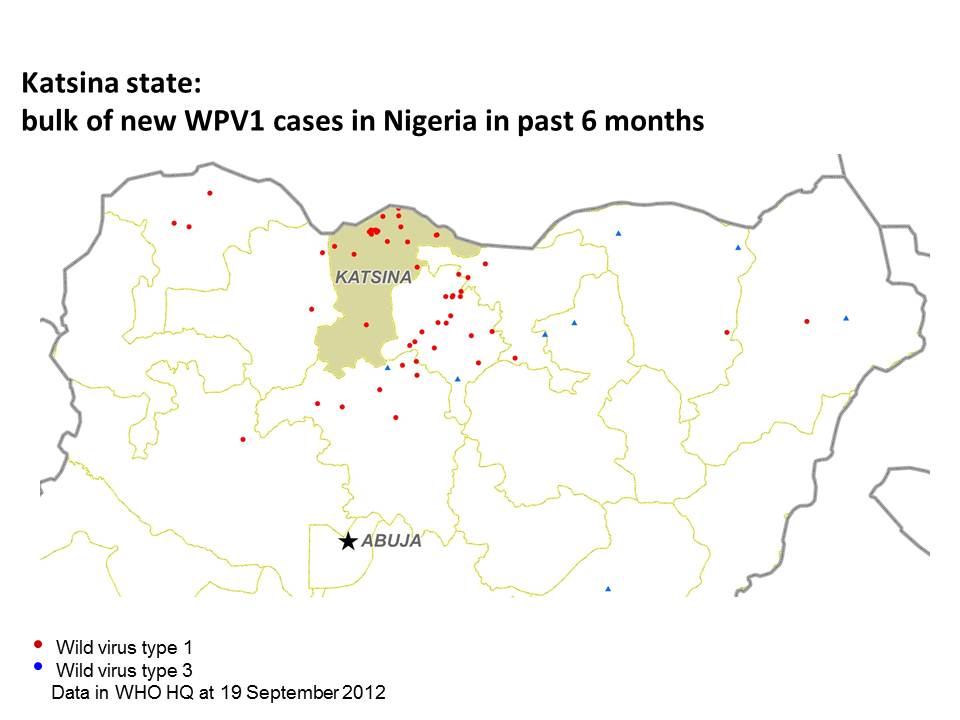
21 September 2012 – Urgent efforts are underway to stop an outbreak of wild poliovirus type 1 (WPV1) in the northern state of Katsina, Nigeria. Over the past six months, Katsina reported 18 WPV1 cases, accounting for 40% of the entire country’s WPV1 burden during that time. In addition to the impact on Nigeria’s eradication efforts, health officials are extremely concerned that the outbreak could spread across the border into neighbouring Niger.
Upwards of one-third of the state’s 1.3 million children aged less than five years are estimated to be under-immunized. During the July Immunization Plus Days (IPDs), nearly one-third of the target population was missed in Katsina city (the most populous part of the state and location of the bulk of the cases). Emergency efforts are now underway to boost population immunity levels as rapidly as possible, to curb the intense transmission of the virus in the area.
Technical capacity is being scaled up for the upcoming IPDs on 29 September to 2 October. Microplans are strengthened in line with new operational guidelines, and drawing on lessons from recently-conducted IPDs, to more accurately map populations and prepare plans for individual vaccination teams’ daily activities. Planning is focusing on integrating the scaled-up technical capacity into well-functioning units, particularly in known worst-performing Local Government Areas (LGAs). Traditional leaders are further being engaged, and targeted social mobilization increased. Tactical recommendations by surveillance medical officers (SMOs) from India, who had recently observed activities in northern Nigeria, are being fully integrated into preparations. And to reduce the risk of the virus spreading across into Niger, special border vaccination teams will be placed at and near known border crossings.
The activities will be much more closely monitored and evaluated, with field volunteers, independent monitors and supervisors concurrently monitoring individual teams while they still operate during the day. Any identified gaps in quality will then be immediately rectified by the individual teams, on the very same day. It is a significant shift in how monitoring, and subsequent implementation of necessary corrective measures, was conducted previously.
Ultimately, however, key to success will be the full and consistent engagement of the political leadership at the LGA level. To help ensure this, His Excellency the Governor of Katsina Ibrahim Shehu Shema expressed his commitment to securing stronger engagement and ownership by LGA Chairpersons, through increased accountability for operational quality.
In neighbouring Niger, activities are also gearing up to minimize the risk and consequences of potential spread from Katsina. Immunization campaigns are taking place on 22 September in key border areas, and the country will participate in a broader multi-country immunization campaign with nine other west African countries at end-October.
These measures are critical given the intense transmission in northern Nigeria, and a history of polio spread from there across the region. However, such resource intensive activities cannot be sustained indefinitely, and key to protecting the region in the long-term is to urgently finish the disease once and for all in Nigeria.
A child in northern Nigeria learning in a Tsangaya, or Koranic school UNICEF / Nigeria
JIGAWA (Nigeria), 29 August 2012 –To address the current upsurge of polio cases in Nigeria, UNICEF, with the support of the US Centers for Diseases Control and Prevention (CDC), and partners, is set to join hands with Koranic school teachers. Early in September, the Tsangaya School Strategy will be piloted in 10 high-risk local government areas (LGAs) of Jigawa and Zamfara states, to reduce the number of missed children during polio campaigns and help build community ownership of immunization.
“We continue to miss too many children during polio campaigns in Nigeria and that is why we continue to have cases,” said Paryss Kouta, UNICEF Chief of Polio Communication a.i. in Nigeria. “Koranic school teachers, or Tsangaya teachers, have an important role to play in ensuring each and every child is reached during polio campaigns given the fact that many children can be found in their schools. Engaging religious schools, institutions and leaders will help build community ownership for immunization and help reduce on-going misconceptions and resistance to immunization.”
The Tsangaya School Strategy involves the full engagement of religious school teachers who are community leaders and opinion-makers in their communities. For polio eradication to succeed, it is important to engage and ensure the full participation of all sectors of society and in particular the communities themselves.
Advocacy meetings and sensitization workshops will be organized with high-level policy makers, traditional and religious leaders, including the Association of Proprietors of Koranic Schools in each of the participating LGAs. Tsangaya teachers will also be engaged during immunization campaigns as part of the social mobilization teams within their respective settlements for the purpose of convincing those households which may refuse immunization.
This project will also engage Preachers and Imams, especially during Friday Mosque sessions to ensure the community is fully aware of the importance of immunization during every campaign and the risks to children who are not immunized. Rallies with school children and other awareness activities will be further organized at the community level in each of the participating LGAs.
Vaccinator administering the Oral Polio Vaccine during the May 2012 Immunization Plus Days UNICEF Nigeria/Andriamasinoro
16 August, 2012 – To stamp out polio in Nigeria, every child must be identified, reached and vaccinated – each and every vaccination round. Every unvaccinated child increases the risk of polio spreading rampantly once more, threatening not only the rest of the country, but the entire importation belt of west and central Africa.
This is why it is worrying that the neighbouring states of Zamfara and Sokoto have had 12 cases of polio this year, compared to only three at this point in 2011. Among the various reasons for this increase in cases, operational difficulties stand out. These are challenges in planning and implementing vaccination rounds, which are preventing children from receiving the polio vaccine.
Reaching huge swathes of people across the large and difficult terrain of Zamfara and Sokoto is far from easy, particularly in round after round of campaigns. Microplans laying out the strategy to reach every last child certainly help, but, to be as effective as possible, they must be repeatedly updated – particularly to take into account the current whereabouts of any of the ten million nomads who circulate through northern Nigeria. Even with these plans in place, reaching every child in the most remote villages can be a daunting task, especially in areas that are inaccessible by road. Vaccination teams and their supervisors must be motivated to travel over difficult terrain time and time again.
But sometimes the reason why children miss out is much simpler – they just aren’t at home when the vaccinator calls. Unlike in many countries, children in states such as Zamfara and Sokoto are not always found with their mother or father. Instead, children as young as three can be sent out to herd cattle on their own or are looked after at the playground by brothers or sisters, who are, themselves, sometimes as young as five years of age. In Sokoto, for example, 32% of children who were absent from the house in the September 2011 vaccination campaign were at the playground, 27% were in the fields, and 19% were attending a social event with their mother or father.
The programme is tackling these operational difficulties with fresh ideas. Microplanning strategies have been refined, using lessons learned from India’s successful eradication programme. Mapping and oversight have been improved by the introduction of GPS and mobile technology. The ‘Nomad Project’ is producing plans to reach nomadic populations with both the vaccine and tailored communications. And vaccinators who consistently reach a high percentage of children will be recognised and rewarded, hopefully inspiring those on the ground to keep trying their hardest.
Importantly, hardworking polio personnel are also having their loads lightened by a 300% increase in human resources. In the last two months, 2,000 new staff have been trained, expanding the programme’s overall capabilities.
These changes are intended to re-energize, improve and refresh the programme, so that the last remaining children will receive their drops of polio vaccine too.
Polio immunizations in refugee camps Rotary International/JM Giboux
West Africa just comes off the heels in stopping a multi-country polio outbreak that affected 12 countries from 2009 to 2011, caused 281 cases and cost US$94 million to control. But the threat of a renewed outbreak now looms as large as ever.
West Africa has traditionally always been at risk of polio re-infection. Together together with a band of countries in central Africa and the Horn of Africa, west Africa forms what is collectively known as the ‘poliovirus importation belt’. Since 2003, more than 60 polio outbreaks have occurred in this importation belt. But this year, the threat of another multi-country outbreak is further magnified, due to a number of critical factors.
First and foremost, polio transmission is this year again intensifying in northern Nigeria, and it is from here that historically polio has spread into Niger, Mali and further into west Africa. Second: the entire region is seeing large-scale population movements, due to insecurity in Mali, the Sahel crisis and the upcoming rainy season – these movements could easily transport the poliovirus right back across the entire region. And finally, a lack of funds this year has forced the cancellation or scaling back of key immunization activities in 24 high-risk countries, including in many areas of west Africa. This is leaving more children there needlessly vulnerable to polio.
The key to urgently minimize the risk and consequences of renewed polio spread in the region is to boost immunity levels. Therefore, ahead of the rainy season, all available resources were prioritized, and from 29 June to 2 July, immunization campaigns took place in the very highest-risk areas of Niger, Mali, Burkina Faso and Guinea.
And at the same time, oral polio vaccine (OPV) is also being integrated into other humanitarian response activities the region. UNICEF in particular is leading a strategic body of work to provide OPV into an integrated response package right across the Sahel and Mali crises region. Working with the UN Refugee Agency UNHCR, the World Food Programme (WFP), other UN organizations and non-governmental organizations (NGOs), activities are focusing on nutrition, health (including vaccination, treatment of pneumonia and diarrhoeal diseases and distribution of bed-nets), and behavior change communication (promoting hygiene and sanitation, infant and young child feeding, etc). Immunization campaigns continue to occur in refugee camps in countries bordering Mali, including in Mauritania and Burkina Faso, and in internally-displaced persons camps in Mali itself. And population movements are actively tracked and mapped, with health posts set up at key border crossings, gathering sites and in hard-to reach areas.
These measures are the bare minimum which must be implemented, but they are opportunistic – ideally, all areas across west Africa should further boost immunity levels in a synchronized and concerted manner to urgently address the risk of a new polio outbreak. Discussions are underway for multi-country, synchronized immunization campaigns in the region later in 2012. Such activities were critical in successfully stopping the 2009-2011 outbreak. However, dependent on implementing such campaigns will be the availability of funds – and currently, the Global Polio Eradication Initiative (GPEI) continues to face a dangerous funding gap of US$945 million.
The Independent Monitoring Board (IMB), established to evaluate progress towards a polio-free world, in its most recent report underscored the potential consequences associated with this lack of financing, which it called ‘not compatible with the ambitious goal of stopping polio transmission globally.’ The IMB repeatedly expressed concern at the cuts of vaccination campaigns which are being made as a result of the ongoing funding gap and the risk this poses to children in particular in west Africa. Unless the funding gap is urgently filled, the specter of yet another multi-country outbreak could well end up costing much more – not just financially, but more importantly, in terms of the human cost.
Polio is at its lowest levels since records began, with fewer cases in fewer districts of fewer countries than at any previous time. But the risks of the disease coming back are grave. Mathematical modeling predicts that failure to achieve success now could result in as many as 200,000 new cases every year, within ten years, all over the world.
To prevent this humanitarian catastrophe, much depends on ensuring the needed funding is urgently made available.
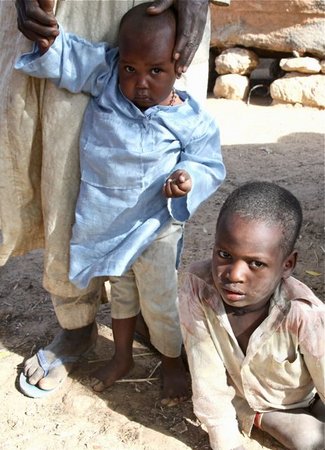
Little Tukur Bello (right) and his older brother Abdullah are from Zamfara State, Nigeria. They are both bright and alert and enjoy playing with each in the small and remote community in which they live. Tragically, both of them are paralyzed by polio.
Five years ago, Abdullah fell sick with fever along with two of his brothers. Both his brothers died and Abdullah has never walked again.
Polio returned to their village in late 2010. Sadly, Tukur Bello had not received any doses of routine immunization and just one dose from a recent campaign. He became the latest victim in this small community to be permanently affected.
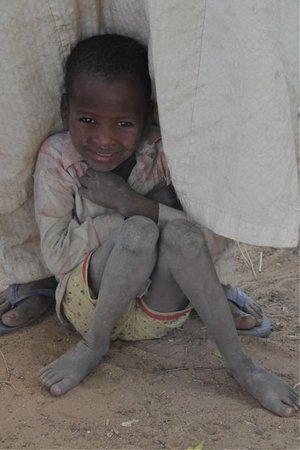
It is three months now since Tukur Bello fell ill. Fortunately the polio virus has attacked the nerves in one leg and Bello can still stand.
His brother Abdullah has not been so lucky and must crawl through the dirt on his knees to move around the settlement.
His brother is lively and inquisitive. However, his legs are too weak to carry .
In the village, Bello is still coming to terms with falling sick and the attention it still brings. He is very shy.
It is a busy day in the village and everyone has come out to see the visitors. It is the first national immunization plus day for 2011 and additional focus and attention is being made to ensure all children in the community are reached with both oral polio vaccine and measles vaccine as part of an integrated campaign.
One Village, Five lives
Older girls bring many of their younger brothers and sisters.
It is loud and chaotic as the children gather round the health workers.
Importantly fathers also bring children to the post for immunization.
Bello is fascinated at what is going on and gets a closer look.
He is almost lost in the crush.
He is almost lost in the crush.
An additional dose of bivalent oral polio vaccine is given to all children under five.
And a shot of measles vaccine is also given to all children between 9 months and five years.
One Village, Five lives
As the last children arrive at the post and as the health workers begin to pack up to move to the next village.
Attracted by the noise and commotion another child arrives at the immunization post. From a neighbouring settlement, Muhammad was also paralyzed five years ago at the same time as Abdullah.
Brave and strong but with the need of a permanent crutch to help him walk, Muhammad is just one more reminder of the devastating affect this virus has had on local families.
It is these three children who leave a lasting impression.
On their way homeward.
One Village, Five lives
I realize like my memories, their paralysis will be with them always. One village, five lives devastated.
Northern Nigeria is one of the last areas in the world with endemic poliovirus.
In 2008, 798 children were paralysed by polio in Nigeria – more than any country in the world. This is because not enough children are vaccinated.
Once a child is paralysed by polio, it is for life. There is no cure.
There is a solution to ending polio. The oral polio vaccine is safe and effective and has successfully stopped polio in over 190 countries.
Vaccinating every child under five years old builds population immunity. If every child is protected, the virus can no longer survive.
To reach every child, adequate vaccine and logistics must be sourced and distributed to local government cold stores.
Each and every village in Nigeria must be accurately mapped to show all households.
Teams must be trained to vaccinate around 41 million children under five years old.
Just as important, parents must be told of the threat that polio presents to their children, and how to protect them.
Politicians and law makers must visibly support vaccination campaigns and commit themselves publicly to eradicating the virus.
Success in other countries has proven time and time again that we have the tools to finish the job.
So take a moment to think about how lucky you are to have the full use of your arms and legs, and put your hand up for polio eradication!
Together we can “KICK POLIO OUT OF NIGERIA FOREVER”.
Nigeria
Nigeria
Nigeria
Nigeria
Nigeria
Nigeria
Nigeria
Nigeria
Nigeria
Nigeria
Nigeria
Nigeria
Nigeria
Vaccinators check their plans before heading out with a cooler box with vaccine to immunize children. UNICEF
On 7 July 2012, Angola achieved a significant milestone – a year without a single case of polio. Its last case dates to 7 July 2011, from Uige province, and was a new importation from neighbouring Democratic Republic of the Congo (DR Congo). Angola’s last indigenous case due to its re-established transmission virus dates back to March 2011.
This fantastic achievement is the result of the dedication of the Angolan people and their government to reach children everywhere with oral polio vaccine (OPV). Provincial Governors and Local Administrators have been empowered to take charge of polio eradication within their communities – a strategy which has paid off handsomely, as improved vaccination coverage figures in rural areas show. Additionally, the Government of Angola funds nearly 90% of current operational costs for polio eradication, and strong commitment is evident at all levels, including by His Excellency President José Eduardo dos Santos, and the Honourable Minister of Health Dr José Vieira Dias Van-Dúnem.
However, this does not mean that the country can breathe a sigh of relief and let down its guard, as many children in the capital, Luanda, and the greater province surrounding it, continue to miss out on receiving OPV. In its most recent report from June 2012, the Independent Monitoring Board (IMB) in particular highlighted ongoing risk to Luanda, which it calls the ‘natural home for polio’ in the country and where ‘poor surveillance and unacceptable levels of missed children are putting Luanda at high risk’. Independent monitoring data indicates that upwards of 10% of children are missed during supplementary immunization activities (SIAs). Many areas are not always reached by the public health services in Luanda. In addition, most of the health workers are overburdened with other competing priorities at operational level.
And so, while in early 2011 Luanda was seeing independent vaccination campaign monitoring results with less than 10% of all children being missed, in more recent campaigns most municipalities have consistently reported well above this figure as having missed out. Several reasons for missed children were identified including the poor selection of vaccinators and supervisors, the inadequate training of vaccination teams, the insufficient supervision and the weak microplanning. In some municipalities of Luanda, a loss of committed leadership of local Administrators was also observed, in leading the all-out process of polio campaign preparation and supervision. As a result, a significant number of houses were not visited by the vaccination teams during the campaigns in Luanda province (‘house not visited’ accounted for above 50% of the reasons for missed children during the last three polio campaigns in Luanda, per independent monitoring data).
To counteract this, UNICEF and WHO are working with the International Committee of the Red Cross and faith-based groups to build support for the programme among local leaders including the churches. WHO staff represented in the 18 provinces, the STOP team and international consultants from the US Centers for Disease Control and Prevention (CDC) are also providing technical support to local authorities to help them prepare and carry out vaccination campaigns. With the financial contributions from the Angolan Government to WHO – US$ 5 million – to support the implementation of the polio emergency plan 2012-2013, WHO has recruited additional national health workers for Luanda province to ensure a more manageable workload. So, since April 2012, each of the 11 municipality of Luanda is now supported by a health technician with a vehicle and driver from WHO to conduct additional training to vaccination teams and their supervisors, to review the campaign microplans and provide intensive supervision during the implementation. The Angolan government with the support of the international agencies and the local partners is also committed to plan and implement mop-up campaigns in order to vaccinate the missed children identified through the post- campaign independent monitoring.
Ensuring that vaccination teams reach all the children of Luanda’s slums will be crucial if Angola is to remain polio-free and stave off a re-importation of the poliovirus. And as long as polio continues to circulate elsewhere – including in nearby Nigeria, Chad and neighbouring DR Congo – re-importation remains a very real possibility. Angola had originally defeated polio in 2001 but has suffered repeated re-importations since 2005. In order to avoid a repeat of past polio resurgences, the country will now have to work hard to ensure that all Angolan children, including those living in and around Luanda, and in the bordering districts of the country are protected against the disease.
This is the second part of our ongoing series on reaching the last child in the remaining polio ‘sanctuaries’. Read the first part of the series, looking at reaching the last children in Afghanistan, here.
New cases at lowest levels ever, but funding gap threatens progress
Vaccinators during a SIA, Nigeria WHO/T. Moran
Geneva, Switzerland 24 May 2012– Despite the dramatic drop in polio cases in the last year, the threat of continued transmission due to funding and immunization gaps has driven the Global Polio Eradication Initiative (GPEI)to launch an Emergency Action Plan.
The plan aims to boost vaccination coverage in Nigeria, Pakistan and Afghanistan, the three remaining polio endemic countries, to levels needed to stop polio transmission. In parallel, health ministers meeting at the World Health Assembly this week are considering a resolution to declare “the completion of polio eradication to be a programmatic emergency for global public health,” in an acknowledgement of the urgency of the situation.
Polio eradication activities resulted in several landmark successes in 2010-2012. India, long-regarded as the nation facing the greatest challenges to eradication, was removed from the list of polio-endemic countries in February 2012. Outbreaks in previously polio-free countries were nearly all stopped.
Although the number of polio cases was lower in the first four months of this year than during the same period in any other year, cases continue to occur in Nigeria, Pakistan, Afghanistan, and Chad. Outbreaks in recent years in China and West Africa due to importations from Pakistan and Nigeria, respectively, highlight the continued threat of resurgence. By some estimates, failure to eradicate polio could lead within a decade to as many as 200,000 paralyzed children a year worldwide.
“Polio eradication is at a tipping point between success and failure,” said Dr. Margaret Chan, Director-General of the World Health Organization. “We are in emergency mode to tip it towards success – working faster and better, focusing on the areas where children are most vulnerable.”
Once achieved, polio eradication would generate net benefits of US $40-50 billion globally by 2035, with the bulk of savings in the poorest countries, calculated based on investments made since the Global Polio Eradication Initiative (GPEI) was formed and savings from reduced treatment costs and gains in productivity.
“We know polio can be eradicated, and our success in India proves it,” said Kalyan Banerjee, president of Rotary International, a global humanitarian service organization. “It is now a question of political and societal will. Do we choose to deliver a polio-free world to future generations, or do we choose to allow 55 cases this year to turn into 200,000 children paralyzed for life, every single year? ”
Full funding of new plan critical
Already, funding shortages have forced the GPEI to cancel or scale-back critical vaccination activities in 24 high-risk countries. This leaves more children vulnerable to contracting the disease, and exposes polio-free countries to the risk of re-emergence.
“All our efforts are at risk until all children are fully immunized against polio – and that means fully funding the global eradication effort and reaching the children we have not yet reached,” said UNICEF Executive Director Anthony Lake. “We have come so far in the battle against this crippling disease. We can now make history – or later be condemned by history for failing.”
Full implementation of the Emergency Action Plan (EAP) is currently hindered by a critical funding gap of nearly US$1 billion through 2013.
“We are all responsible for creating a polio-free world while we still can,” said Chris Elias, president of global development at the Bill and Melinda Gates Foundation. “Achieving this goal is a critical step in protecting all children from vaccine-preventable diseases.”
The Global Emergency Action Plan
Corbis / KerenSu Two Pakistani Boys in the Hunza Valley
Intensified focus on worst-performing areas of Nigeria, Pakistan and Afghanistan to increase vaccination coverage by end of 2012 to levels needed to stop transmission;
• New approaches tailored to each country to tackle persistent challenges and improve polio vaccination campaign performance;
• Heightened accountability, coordination and oversight to ensure success at every level of government and within every partner agency and organization;
• Surge of technical assistance and social mobilization capacity.
Working in emergency mode
We need everyone’s commitment and hard work to eradicate polio and cross the finish line,” said Dr. Thomas Frieden, director of the U.S. Centers for Disease Control and Prevention (CDC). “It won’t be easy, but together we can eradicate polio forever and for everyone.”
Already since the start of the year, the GPEI has moved its operations into emergency mode. CDC has activated its Emergency Operations Center; UNICEF has officially activated an Interdivisional Emergency Coordinating Committee operating directly under the Deputy Executive Director; and WHO has moved its polio operations to its Strategic Health Operations Centre (SHOC). Such measures are reserved for responding to global health emergencies — such as the H1N1 pandemic or the 2004 Southeast Asia tsunami — and will enable a massive surge in technical capacity, real-time tracking of program performance and the immediate implementation of corrective action plans as necessary. Also this year, the Trustees of the Rotary Foundation reaffirmed polio eradication as the organization’s most urgent priority. In addition, Rotary senior leaders have launched a series of one-on-one meetings with the heads of state of the polio endemic countries.
UN Secretary-General visits the polio-affected country
As he gave oral polio vaccine to an Angolan child, the UN Secretary General quipped, “The vaccine is easy to administer. Even I have done it!” Quintiliano dos Santos
29 February 2012 – All Angolans, “health workers, volunteers, mothers and fathers”, must work together to ensure that polio is eradicated and to prevent the country from being re-infected once more– this was the message UN Secretary-General Ban Ki-moon shared during his recent visit to the country.
At the launch of Angola’s National Immunization Days in the capital, Luanda, on 27 February, the Secretary-General told on-lookers “Polio should be tackled as a public health emergency.”
Eradicating polio is one of the Secretary General’s five health priorities for his second term. Ban Ki-Moon also pledged sustainable solutions to improve the supply of drinking water and environmental health to mitigate the risk of water-borne diseases like polio, stressing that Angola leaders understand this priority.
“Efforts to eradicate polio in Angola are on track” he said while paying a tribute to the Government for funding 89% of current operational costs for polio eradication, with a high commitment of the Head of State Jose Eduardo dos Santos.
In his remarks, the Minister of Health, Dr. José Van-Dunem, emphasized the strategy adopted by the Angolan Government to increase the involvement of local authorities and communities in the organization of immunization activities at local level, by ensuring that every house is reached by mobile teams and to conduct synchronized campaigns together with bordering countries.
Despite having previously put a stop to polio transmission in 2001, Angola has been reinfected several times since 2005 and has struggled with ongoing transmission ever since. However, through the dedication of its government (who are financing 88% of the country’s current eradication efforts) and the hard work of its people, Angola has not seen a case since July last year.
Since 2011, Angola has been implementing a new strategy to accelerate the eradication of polio which consists of a greater ownership by provincial Governors, municipal Administrators, and local communities in immunization activities. The new approach also includes local recruitment of vaccinators and supervisors under the coordination of community leaders to ensure that every child is reached during the vaccination campaigns.
The number of wild polio cases in Angola has drastically decreased from 33 in 18 municipalities, in 2010, to 5 cases in two municipalities in 2011.
During a Supplementary National Immunization Days, Kano Nigeria.
The strategy to eradicate the remaining strains of wild poliovirus was discussed at length during the meeting of WHO’s Strategic Advisory Group of Experts on immunization (SAGE) held from 8-10 November in Geneva.
Reviewing the latest global epidemiology, SAGE expressed alarm that the risk of failure to finish global polio eradication constitutes a programmatic emergency of global proportions for public health, and was not acceptable under any circumstances. Failure, SAGE warned, would lead to a major resurgence of the disease with many children crippled for life again every single year. At the same time, it would also represent the most expensive public health failure in history, with far-reaching consequences on overall global immunization efforts, seriously undermining the credibility of public health efforts with donors and stakeholders.
SAGE urged that rapid steps be taken to tighten accountability for programme and individual performance within governments as well as implementing and donor agencies, to ensure that more children are reached during eradication strategies and that the effort is fully financed. “There must be consequences at all levels for individuals, institutions and governments who fail to deliver on their mandate,” SAGE reported.
Given the ongoing international spread of poliovirus from infected areas, SAGE encouraged the application of appropriate vaccination recommendations for all travellers to and from polio-infected areas. At the same time, SAGE stressed that communities and civil societies must be engaged and mobilized to put pressure on governments to ensure that they remain committed to the disease’s eradication. SAGE recommended that polio-infected countries be requested to submit an annual progress report to the World Health Assembly.
The report of the meeting will be published in the WHO Weekly Epidemiological Record on 6 January 2012.
The meeting documents ― including presentations and background readings ― can already be found on the web.
States eligible for US$ 500,000 grant to address pressing health issues
Children in Zamfara State, Northern Nigeria wait to be immunized with OPV WHO/Thomas Moran
SEATTLE — Bill Gates, co-chair of the Bill & Melinda Gates Foundation, announced a new initiative today for Nigeria’s Executive Governors challenging them to deliver a dramatic improvement in polio and routine immunization by the end of 2012.
The program, initiated together with the Nigeria Governors’ Forum, will recognize those Executive Governors whose states pass a pre-defined threshold to improve routine immunization coverage and end polio. The states that meet the threshold criteria will be awarded a US$ 500,000 grant from the Bill & Melinda Gates Foundation to support their top health priorities.
“Nigeria’s leaders are critical to making Nigeria polio free and their renewed confirmation last week of the Abuja Commitments will make an important difference,” said Gates. “As governors push hard over the next year to achieve the 2012 deadline to end polio, I want to ensure their efforts are acknowledged and that the governors are simultaneously supported to tackle other key health problems they face in their states,” said Mr. Gates.
“Nigeria’s governors want to stop polio and improve routine immunization to protect Nigeria’s children against preventable diseases,” said His Excellency Chibuike Rotimi Amaechi, Governor of Rivers State and Chairman of the Nigeria Governors’ Forum. “This award recognizes that effort, and the fact that we need to work hard if we want to stop polio in this country by 2012.”
Gates in Nigeria
Gates was in Nigeria last week to discuss polio eradication and immunization with senior government leadership in Nigeria. He met with President Goodluck Jonathan who announced a special task force to spearhead the federal effort to support states in stopping polio. He also observed as their Excellencies Vice President Namadi Sambo and Governor Amaechi signed a communiqué adopting and re-confirming the 2009 Abuja Commitments. Those commitments lay out clear steps for Executive Governors and Local Government Area Chairmen to ensure that polio is stopped and immunization services are reaching more children.
And in Chad
With President Idriss Déby, Gates launched a new polio immunization campaign that aims to immunize the country’s 2.2 million children under the age of five against polio.
The President declared: “On behalf of the people of Chad, and especially mothers and children, we thank Bill Gates for coming to Chad and for his generosity in putting his fortune to the service of children and humanity. Mr. Gates, you are a leader in the fight to eradicate polio worldwide,” he added before concluding his message with a call to action to Chad’s citizens: “By coming to Chad to launch this vaccination campaign, Mr. Gates calls on all of us – the government, large institutions, media, parents, leaders of different religions, traditional leaders, territorial administrations and defense and security – we should mobilize ourselves to eradicate polio.”
Approximately 41 percent of polio cases in Africa were reported in Chad this year, increasing the likelihood of the country becoming a reservoir for the spread of the virus to neighbouring countries. This immunization campaign offers a new opportunity for the country to curb the spread of polio and offer thousands of children a chance to live a life free from life-long paralysis.
“I would like to congratulate His Excellency, President Idriss Déby ITNO and his government for their continued commitment to eliminating polio and giving children a healthy start to life through immunization,” said Gates. “Chad is on a path toward eliminating polio and we are committed to play a part in that journey.”
The polio eradication family is mourning its own. The World Health Organization and UNICEF, two of the spearheading partners of the Global Polio Eradication Initiative, both lost staff in the attack on UN House in Abuja, Nigeria on 26 August.
Mr. Johnson Awotunde was with UNICEF as a specialist in Monitoring and Evaluation. His work was critical for the production, with the government, of the best facts and statistics on the state of children. These are used widely by aid professionals as they assess need and decide where to place resources. He leaves a widow and six children.
Mr. Ahmed Abiodun Adewale-Kareem was a logistician at UNICEF and developed particular expertise on the safe importation of vaccines for mass immunisation campaigns. The trust he had established with officials and his ability to ensure the delivery of millions of doses has underpinned the success of immunisation campaigns across the country. He was married with two children. Mr. Adewale- Kareem died when he left his office to meet Mr. Sunday Ekere James, a Shipping Agent who was also killed when he arrived to pick up papers regarding a new polio campaign. Over the years, Mr James worked closely with UNICEF and was the first choice to help ensure the safe arrival of critical commodities.
Dr Edward Dede worked with WHO as National Professional Officer, Routine Immunization. His significant contribution to strengthening routine immunization, polio eradication and other accelerated control of vaccine-preventable diseases was not limited to Nigeria. Dr Dede contributed to several regional initiatives including the updating of the AFRO Expanded Programme on Immunization regional mid-level management modules. Between October 2010 and April 2011, Dr Dede provided technical support to the polio eradication effort in Luanda province in Angola. Moments before his death, he had been inaugurated as the President of the WHO Nigeria Staff Association for 2011-2013. He leaves behind a widow and two children.
Engineer Musa Ali worked with WHO as the Zonal Logistics Assistant for the North West Zone, based in Kano. He ensured the smooth running of WHO operations, including security, staff movements and overall logistical issues within the North West Zone, which includes most of the polio high-risk states in the country. Engineer Musa’s excellent performance contributed to the significant reduction in polio burden in recent years. Just before his death, he had been elected Vice President (North West Zone) of the WHO Staff Association. He leaves behind a widow and three children.
Prince Abraham A. Osunsanya was instrumental at WHO in boosting donor confidence through strengthening the administration of immunization programmes to save and improve the lives of children in Nigeria. He leaves behind a widow and two children.
The event claimed the lives of 23 people including these three staff from WHO and two from UNICEF, and injured many more. Four WHO staff and two UNICEF staff are among the critically injured. The immediate priority is to ensure the care of those injured and to support the surviving staff and the families of the bereaved.
WHO and UNICEF have no intention of curtailing their work with Nigeria and are working around the clock to counsel the bereaved, ensure care of the injured and maintain operations. Together with our partners, we remain committed to the eradication of polio in Nigeria and ensuring that its children will have a future free of the scourge of polio.
Polio eradication was a hot topic at the 38th Session of the Council of Foreign Ministers of the newly renamed Organisation of Islamic Cooperation (OIC – formerly known as the Organisation of Islamic Conferences).
A resolution resulting from the session urges, among other things, that “the member states affected by polio, AIDS, tuberculosis and malaria … undertake necessary steps to fight these dangerous communicable diseases and requests the potential donors to give generously to the GPEI [Global Polio Eradication Initiative] and the Global Fund”.
The resolution also recognizes the ongoing efforts by Afghanistan, Nigeria and Pakistan to eradicate polio, reminds the other member states to ensure their children are immunized against the virus, and requests that the Islamic Development Bank consider funding polio vaccine for Afghanistan.
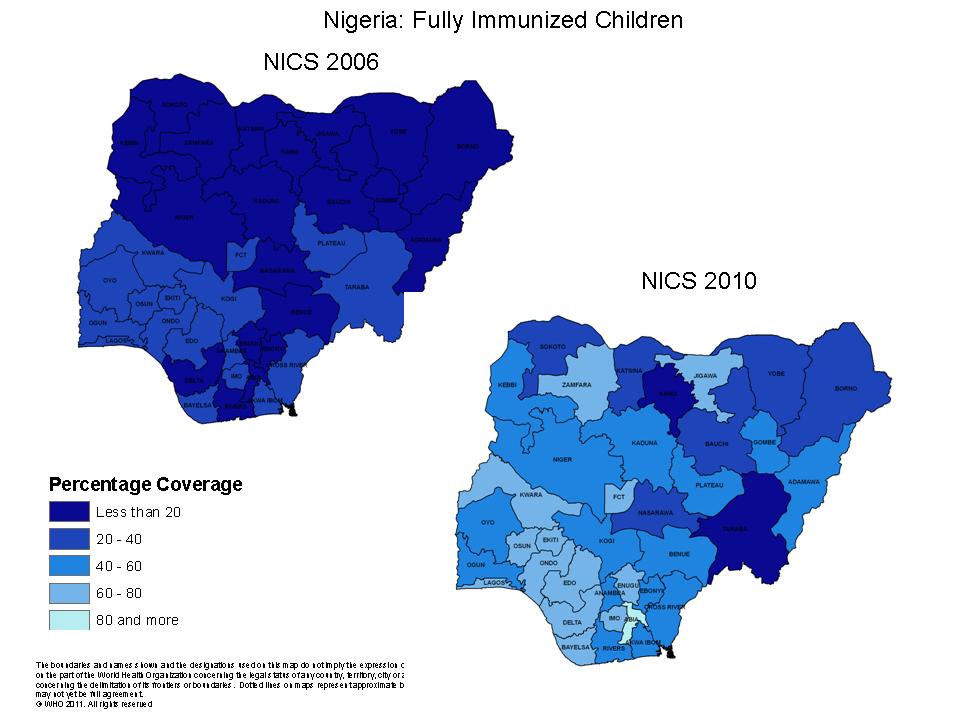
1 June 2011 – Nigeria has nearly tripled the proportion of children covered by routine immunization between 2006 to 2010, according to a new national study. The increase took place against the backdrop of aggressive supplementary immunization campaigns to eradicate polio.
The results of the National Immunization Coverage Survey (NICS), conducted in October 2010, indicate that 52% of Nigerian children aged 12-23 months are reported to be fully immunized, compared with just 18% in 2006. In 2003, when the first baseline study was undertaken, the corresponding figure stood at just 13%.
The study results clearly demonstrate how routine immunization services can be improved in a polio-endemic country even during frequent supplementary immunization rounds. In Nigeria, these mutually beneficial results are due to the strong leadership of Nigeria’s National Primary Health Care Development Agency (NPHCDA).
The results come at a critical time in the efforts to eradicate polio from Nigeria, with just 21 cases of the paralytic disease recorded in 2010 and eight in the first quarter of 2011 – the lowest number of cases ever-recorded. Global health leaders at the World Health Assembly in May 2011 acknowledged these gains.
The survey demonstrates that coverage of routine immunization contributes to the interruption of poliovirus as well as the sustained protection of children against other vaccine-preventable diseases. In individual states and zonal areas of southern Nigeria (in Nigeria’s administrative structure, several states form a ‘zone’) where delivery of routine immunization services is strongest, transmission of poliovirus has been stopped. In northern states, where coverage is lower, polio continues to paralyse children. In 2010, more than 50% of children paralysed by wild poliovirus had never received a dose of polio vaccine despite intensified efforts.
NPHCDA supported state and local government authorities to implement the approach known as ‘Reaching Every Ward’, which facilitates comprehensive coverage. Polio campaigns are used to disseminate key messages about routine immunization. In several states, polio campaign micro-plans – the detailed plans which drill down to the individual home level to ensure all children are vaccinated – have been adapted to support delivery of routine immunization services. Task Forces that support implementation of polio eradication activities in the highest-risk States and Local Government Areas include strengthening of routine immunization in their terms of reference: this too has contributed to the progress being registered
The NICS aims to estimate the levels of immunization coverage at national, regional and state levels. The survey is regarded by the Nigerian Government and international partners as the most accurate measure of routine immunization services, providing important insights into community and individual attitudes towards immunization.
More than 19,000 households in selected settlements of every state were visited in October 2010 by trained representatives of an independent research company. Coverage was determined by vaccination card and the child’s history as recounted by the family at 52 weeks of age.
Coverage of DPT3 – a measurement of the number of children who are fully protected against three killer diseases Diphtheria, Pertussis and Tetanus and the most common measurement of basic routine services – increased nationally from 25% in 2006 to 68% in the 2010 study. Advances were recorded in all regions of the country.
This progress in Nigeria is tempered by the survey finding that almost one in four children do not receive any routine immunization. The country’s ability to bring this figure down will determine whether or not Nigeria can interrupt polio and deliver on its pledge to meet health-related Millennium Development Goals by 2015.
As part of efforts to prepare for the polio post-eradication era, the World Health Organization (WHO) and its partners have facilitated the development and transfer of new polio vaccine technology to vaccine production facilities in India and the Republic of Korea.
In collaboration with the Netherlands Vaccine Institute (NVI), and more recently the National Institute for Public Health and the Environment (RIVM) in the Netherlands, clinical lots of inactivated polio vaccine (IPV) produced from Sabin poliovirus seed-strains have been prepared. Traditional IPV is manufactured using wild poliovirus and an inadvertent biocontainment failure could be associated with serious consequences in some areas of the world in the post-eradication era (ie areas with high population density, inadequate sanitation infrastructure and low population immunity levels). Sabin seed strains for IPV have the advantage over wild polioviruses that they are attenuated, and hence are safer for handling and IPV production in developing country settings in the post-eradication era.
In this first phase of a broader intended technology transfer programme, two manufacturers have been selected to receive this new technology for vaccine production: Panacea Biotech, Ltd in India, and LG Life Sciences, Ltd in the Republic of Korea. Both manufacturers have confirmed their intention to use all reasonable efforts to apply for registration of their Sabin IPV products in the country of production within four years from the dates of conclusions of the bilateral agreement with RIVM. WHO and RIVM will continue the technology transfer programme this year with further manufacturers.
This transfer of technology is a significant milestone in preparations for the polio post-eradication era. Following the eradication of wild poliovirus globally, use of all oral polio vaccine (OPV) in routine immunization programmes will need to be stopped due to the risks associated with the continued administration, in the post-eradication era, of the live (attenuated, but not inactivated) polioviruses contained in OPV. These risks include vaccine-associated paralytic polio and the generation of new, circulating vaccine-derived polioviruses. Therefore, after the eradication of all wild polioviruses, and the eventual cessation of OPV for use in routine immunization programmes, any country choosing to continue to immunize its population against polio will need to do so with IPV, the only option which will be available to do so at that time.
Recognizing that the manufacturing costs and price of IPV are currently substantially higher than that for OPV, the Global Polio Eradication Initiative (GPEI) is studying a range of approaches to establish affordable strategies for IPV use in low-income settings following OPV cessation. The development, manufacture and distribution of a safe, effective and affordable Sabin IPV that can be produced securely in developing country settings is a key landmark in this programme of work. This technology transfer will also help to boost more broadly the domestic production capacity for vaccines and the strengthening public of health systems to ensure more equitable access to vaccines.
The development of Sabin IPV and the related technology transfer work has been generously supported by the Bill & Melinda Gates Foundation.
The GPEI is spearheaded by national governments, WHO, Rotary International, the US Centers for Disease Control and Prevention (CDC) and UNICEF. Since 1988 (the year the GPEI was launched), the incidence of polio has been reduced by more than 99%. In 1988, more than 350,000 children were paralysed each year in more than 125 endemic countries. In 2010, 1,291 cases were reported worldwide, from 20 countries. Only four countries remain endemic: Afghanistan, India, Nigeria and Pakistan.
The global health community signalled strong commitment to polio eradication this week, underlining the financial needs to finish the job.
Delegates in one of the committee meetings held during the World Health Assembly 2011 WHO/Pierre Albouy
24 May, Geneva – Delegates at the World Health Assembly (WHA) focused on the ‘significant advances’ since the launch of a new strategic plan and new, bivalent oral poliovirus vaccine in 2010. In India and Nigeria, the source of all importations of wild poliovirus into previously polio-free countries in recent years, polio cases declined by 95% between 2009 and 2010; during the same period polio cases due to the type 3 virus declined by 92% globally.
Delegates called for strong national and sub-national leadership by political authorities for the implementation of polio eradication strategies and highlighted the need for countries to significantly strengthen routine immunization.
Delegates expressed particular concern over the funding gap of US$ 665 million to fully carry out polio eradication activities in 2011 and 2012. Several delegates called for levels of political and financial commitment to be sustained until the job is done, reminding the Assembly of the estimated minimum financial benefits of eradication over the next 25 years of US$ 40-50 billion, primarily to low-income countries.
Both donors and polio-affected countries highlighted the resources they were making available and called on others to step forward.
Delegates requested WHO to provide additional technical support to countries with ongoing, re-established polio transmission (Angola, Chad, Democratic Republic of the Congo), to continue to pursue research for post-eradication risk management and to help countries maintain high-quality surveillance and population immunity until eradication is complete globally.
A week before, in her opening address to the WHA, WHO Director-General Dr Margaret Chan told the assembled Health Ministers of the world, “We have been encouraged by a 95% drop in cases in India and Nigeria. But the job is not yet finished and we must see this through to the end.”
Bill Gates, Co-chair of the Bill & Melinda Gates Foundation, was one of the keynote speakers at the Assembly. He reminded global health leaders that the long fight to end polio “demonstrates that technology is only as effective as the leaders delivering it.” He challenged health authorities to reach every child with vaccine and donors to fund the final steps of polio eradication.
The WHA delegates’ discussion came a week after Margaret Chan and Bill Gates met with high-level representatives of polio-affected and donor countries to discuss actions in response to the report of the Independent Monitoring Board. More
New $60 million credit will support major immunization effort during a critical year.
WASHINGTON, March 17, 2011 – The World Bank’s Board approved today an additional credit of $60 million for Nigeria’s Partnership for Polio Eradication project. These funds will help finance polio vaccines during the coming year as well as continue to support other aspects of primary health care in the country.
A comprehensive effort against polio supported by the World Bank and other partners has contributed to a dramatic 95% reduction in polio cases from the year 2009 to 2010. However, detection of even a few new cases in 2010 means that immunization must continue to consolidate these gains.
“The few remaining cases of polio in Nigeria still represent a threat to global fight against polio, as the virus knows no borders and could still spread into more countries,” said Onno Ruhl, World Bank Country Director for Nigeria. “Building on recent gains, the time is ripe to try to wipe out the disease from Nigeria for good through continued immunization, and move a step closer to regional and global eradication.”
In 2011, with the support of the World Bank financing, over 400 million doses of oral polio vaccines will be procured for the supplemental immunization activities at national and sub-national levels and mop-up rounds. Partners’ and government financing will also cover the operational costs for these campaigns and support activities like social mobilization and capacity building. Full press release.
A GIS device is attached to a vaccine carrier bag – Photo by Vince Seaman, US Centers for Disease Control and Prevention (CDC)
As part of ongoing efforts to further improve operational quality of supplementary immunization activities (SIAs), a pilot study was carried out in Nigeria in November to determine the feasibility of using Geographic Information Systems (GIS) to support both implementation and monitoring of SIAs. GIS is a tool that captures, stores, analyses and presents data linked to location(s). The technology has been applied widely in such fields as archeology, geography, cartography, urban planning and land surveying.
Five vaccination teams in Karu ward, AMAC Local Government Area in the Federal Capital Territory were equipped with GIS devices, which tracked and mapped the teams’ movements during the day, in relation to pre-prepared microplans. Analysis of the real-time data allowed for the immediate identification of possible missed areas, which were subsequently re-visited by the teams.
With the initial pilot demonstrating that GIS is useful to improve microplan development and implementation, the initiative will be scaled-up in early 2011 across high-risk areas of northern Nigeria. Successful application could also lead to integration of the new approach to key outbreak areas, including central Africa (Angola, Democratic Republic of the Congo and the Republic of Congo), where the quality of outbreak response has been hampered by operational issues. In the meantime, other pilot studies in Nigeria are exploring a range of new approaches to further sensitize tactics, including the use of Global Positioning Systems (GPS)-enabled mobile phones in end-process monitoring; network analysis to understand and address non-compliance; and, the establishment of local cross-function teams to monitor and rapidly improve SIA performance
In the past two decades, polio cases around the world have been reduced by 99 percent. If we can get rid of the last 1 percent, polio will become the second major infectious disease, after smallpox, that has ever been completely eliminated. There are still gaps in funding for polio eradication, and new outbreaks could reverse some of the progress made so far. But if polio is eliminated, never again will a child be crippled by this terrible virus.
Northern India and northern Nigeria are two areas where polio continues to be a problem. I visited northern India in May this year to see the progress there. I was very excited to visit northern Nigeria in June, because the progress there since my last visit in February 2009 has been especially impressive. As of July 14th, only five cases due to wild polio viruses were reported in Nigeria this year, versus hundreds last year.
I spent most of my first day in Kano, one of the northern states most vulnerable to polio. I met with community leaders, visited a local health center and stopped in at an informal school where students study the Koran in Arabic. On the streets and most everywhere else we went, I noticed so many young children around. Nigeria has more people by far than any other African country, and more than 40 percent of them are under the age of 15. That makes polio immunization a big challenge. Kano had just begun a campaign to immunize more than 6 million children under the age of five.
Part of the challenge is overcoming fear and suspicion. In Kano in the past, false rumors linked immunization to sterility and HIV. Community leaders told me that because polio vaccine is free and brought to people in their homes, some people think there must be something wrong with it. Community leaders play a critically important role in helping to overcome mistrust, and a big focus of anti-polio efforts is on informing these leaders and enlisting their support.



























































 The polio eradication family is mourning its own. The World Health Organization and UNICEF, two of the spearheading partners of the Global Polio Eradication Initiative, both lost staff in the attack on UN House in Abuja, Nigeria on 26 August.
The polio eradication family is mourning its own. The World Health Organization and UNICEF, two of the spearheading partners of the Global Polio Eradication Initiative, both lost staff in the attack on UN House in Abuja, Nigeria on 26 August.