
Emergency appeal for Congo polio outbreak
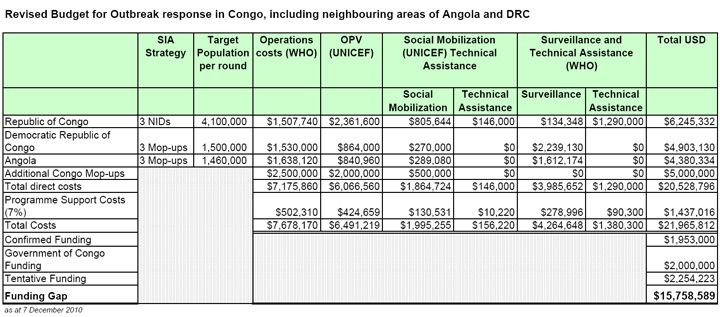
US$ 22 million urgently needed for outbreak response in Congo — appeal from WHO, UNICEF and Rotary International.

Melissa Corkum/UNICEF
Download full appeal (pdf):
English ¦ français
Current Situation:
As of 7 December, at least 476 cases of acute flaccid paralysis (AFP) and 179 deaths have been reported from the site of the acute poliomyelitis outbreak centred in Pointe Noire, Republic of Congo. Six cases have been confirmed to have been caused by wild poliovirus type 1 and laboratory testing continues. Initial data indicates the majority of the reported cases and deaths involve young adults aged 15-25 years. Nearly all cases have been reported from the port city of Pointe Noire, with cases also reported from Niari, Bouenza, Brazzaville, and Kouilou. New cases continue to be reported.
Genetic sequencing of the poliovirus detected has determined that the polio cases are caused by a poliovirus most closely related to that circulating in neighbouring Angola. Congo had recorded its last case of indigenous polio in 2000.
Significance and Risks:
Stopping the outbreak in Congo is a top international public health priority due to the explosive, deadly nature of the outbreak and the high risk of further national and international spread. As well, given that polio is a disease slated for global eradication and the recent progress in Nigeria (98% reduction in cases in 2010 compared to the same period in 2009), rapidly stopping the persistent poliovirus transmission in central Africa (i.e. Angola, DR Congo) and stopping new polio outbreaks such as in Congo, are of critical importance.
The outbreak in Congo is worse than other recent outbreaks of polio due to the extraordinarily high mortality rate seen so far and its explosive nature, with the poliovirus rapidly circulating through a susceptible population. Despite this, experience from other either explosive or adult outbreaks (ex. Namibia, 2006) demonstrates that it can be rapidly controlled if we have the necessary funds to respond appropriately with swift, high-quality vaccination activities. The speed of the outbreak response is vital to stopping the further spread of disease.
Regional Emergency Outbreak Response Activities:
Three elements are central to quickly stopping this outbreak, per the World Health Assembly resolution of 2006: immediate, mass oral polio vaccine (OPV) campaigns with the appropriate type-specific vaccine (a minimum of three such campaigns, and based on other, similar outbreaks, up to eight campaigns, two to four weeks apart); mass OPV campaigns in bordering areas; heightened AFP surveillance in the country and neighbouring areas. The response to the outbreak in Congo also includes all the new innovative emergency response approaches, including the new short interval additional doses (SIAD) strategy, which has increasingly proven to more rapidly stop outbreaks and prevent international spread. Finally, heightened surveillance must be sustained for more than 12 months to ensure that the outbreak has stopped and to guide further actions. Conducting this type of response, though, requires rapidly mobilizing emergency funds.
The Government of Congo has alerted the public to the outbreak and launched an emergency response plan, with support from key partners, including WHO, UNICEF, Rotary International and the US Centers for Disease Control and Prevention (CDC). The first vaccination response, using monovalent oral polio vaccine type 1 (mOPV1), was launched by the First Lady of Congo and the Minister of Health on Friday, 12 November, in Pointe Noire and targeted 1.3 million people of all ages and covering the whole population of Porte Noire and Kouilou, in conjunction with the neighbouring province of Cabinda in Angola and 16 districts in the neighbouring province in DRC. The remainder of the country (target: approximately 3 million) conducted sub-national immunization days with mOPV1 from 18-22 November, which were launched in Brazzaville by the Head of State.
A second nationwide round took place starting 3 December and a third nation-wide round is scheduled for 11 January. Parts of DRC and Angola will also be covered during these rounds, and other neighbouring areas will be monitored and response mobilised as necessary. While full coverage data from the first two rounds is still be analyzed, early indications are that both campaigns were of good quality, with approximately 105% of the target population reached during the first round. As importantly, key lessons learned from the first round were immediately integrated into planning for the second round. These include strengthening the ‘fixed post’ immunization outreach, to facilitate reaching an adult population which may not be at home during house-to-house vaccinations conducted during the day.
The number, geographic extent and target age groups of further campaigns will be determined by the Government based on the evolving epidemiology. The multi-country campaign may be further expanded to cover additional bordering at-risk areas.
Countries across central Africa should strengthen AFP surveillance to rapidly detect any poliovirus importations and facilitate a rapid response. Countries should also address any gaps in polio immunization coverage to minimize the consequences of a poliovirus introduction. As per the recommendations in the WHO publication International Travel and Health to and from all countries where polio is circulating, including the Republic of Congo and Angola, should be fully protected by vaccination.
Funding is urgently needed to ensure emergency response activities can take place. To date, US$6.2 million has been confirmed or is tentative, leaving a funding gap of US$ 15.7 million.
There are five major components of the Global Polio Eradication Initiative budget:
1. Oral polio vaccine supply
In 2009 alone, 2.2 billion doses of vaccine were used to vaccinate children as part of polio eradication efforts. Vaccines are procured by UNICEF. The agency works to ensure that the vaccine supply is secure – with multiple suppliers – and that the price is both affordable for purchase and reasonably covers the needs of the manufacturers.
2. Operational cost of supplementary immunization activities
Supplementary immunization activities are vast operations to deliver vaccine to every household. Detailed maps and plans have to be updated for every dwelling in the area to be covered, vaccines have to be delivered to distribution centres, and vaccinators need to be trained to visit every household and vaccinate every child.
3. Social mobilization and communication:
Experience has shown that it is critical to have strong social mobilization and communication activities planned and implemented prior to immunization campaigns. This requires development of communication plans, involvement of the community leaders and civil societies as well as mass media. Such activities ensure community awareness about the outbreak, planned response and targeted age group. It also secures acceptance to the vaccination efforts and has impact on coverage as community members are mobilized to ensure the targeted age groups are being vaccinated during the each and every round.
4. Surveillance
Surveillance budgets cover the detection and reporting of acute flaccid paralysis (AFP) cases. This is done through an extensive informant network of people who first report cases, and through active searches in health facilities.
5. Technical assistance
When relevant skills are not available within a national health system, staff and consultants are sent to fill the gaps. This extra support helps with immunization campaign planning and implementation, logistics, forecasting and supply management, human resources, communication and social mobilization. Polio eradication staff now constitute the single largest resource of technical assistance for immunization in low-income countries.
Related News




